The Rise of Malaria in Australia Explained
Malaria in Australia
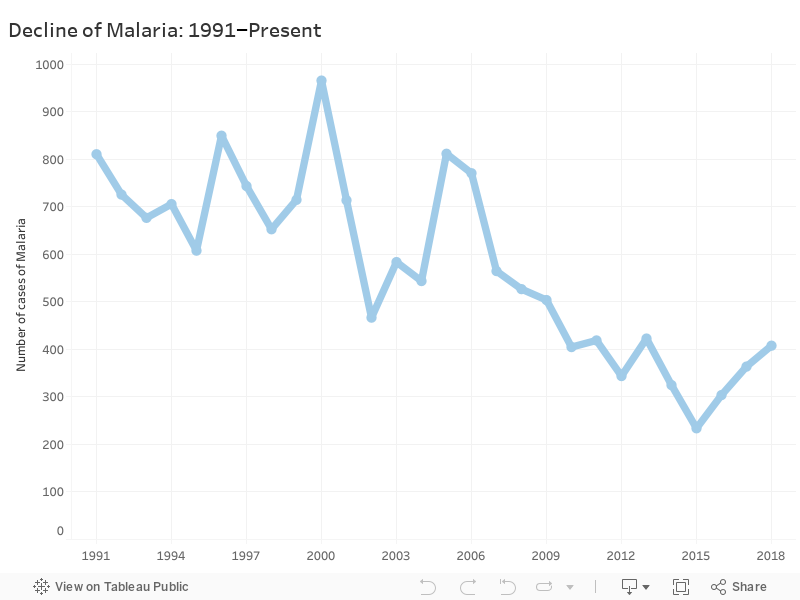
Between 1991 and 2014, cases of malaria in Australia declined. But according to data from the NNDSS, the National Notifiable Diseases Surveillance System, the number of cases of malaria in Australia began to rise from 2015.
Why is malaria in Australia rising?
Dr Cameron Webb, an entomologist at the University of Sydney says that “The change is probably related to a combination of travel undertaken by Australians and changes in activity of malaria in those regions”.
Those regions include (according to the Centers for Disease Control and Prevention) Papua New Guinea, the Pacific Islands, and Indonesia, with the exception of Jakarta, Ubud, Bali, Java, Gili Islands, and Kepulauan Seribu (the Thousand Islands).
Australia has no mosquitos which can infect us with malaria.
“There is no local transmission of malaria in Australia and, officially, we’ve been declared free of malaria by the World Health Organisation since the 1980s” Dr Webb says.
Instead, all instances of Australians infected with malaria are due to travelling. “There are virtually no locally acquired cases these days in Australia but up to 2,000 Australians test positive on return after travel overseas, mostly Indonesia. With malaria, we still see quite a bit of activity in PNG and the Pacific Islands. It is possible that Australians travelling to those regions may have increased for some reason too” Dr Webb says.
“Those cases you see in the notifiable diseases database are all imported cases. These are travellers returning home to Australia and testing positive to malaria infection overseas” Dr Webb says.

This GIF demonstrates the decline of malaria in Australia by state. Notice how Queensland is consistently the most infected state.
Malaria in Queensland
Every year since 1991 (except 2014 and 2016) Queensland had the highest number of cases of malaria.
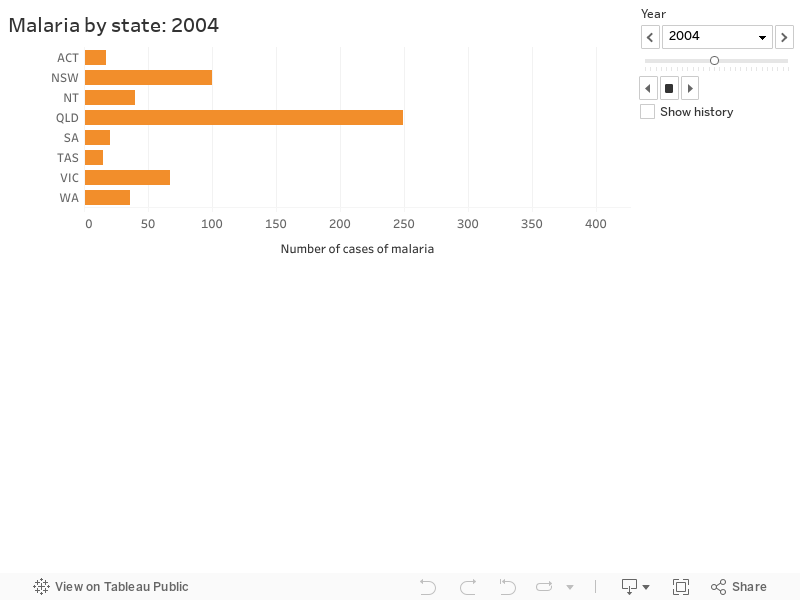
The number of cases of malaria in Queensland was more than double during 1991, 1992, 1995, 1996, 1997, 2003, and 2004.
Queensland has so many more malaria infections than other states because Queensland has more than double the number of Papua New Guinean Australians. It makes sense that Queensland’s number of cases of malaria is usually double.
According to the 2016 census, Queensland has 16,120 Papua New Guinean Australians. New South Wales has the second highest number of Papua New Guinean Australians at 5,466 according to 2016 census data.
More Papua New Guinean Australians in Queensland means more visits to Papua New Guinea where malaria is rampant.
Dr Webb says that “travel overseas to visit friends and family is of greater risk than that of tourist travel. For a few reasons but mostly tourist travel to those locations often take place in resorts where mosquito control is undertaken. Visiting friends or family, individuals may be more likely to be in rural/regional areas without the same level of control. There are likely to be stronger family connections to some communities in Queensland and Papua New Guinea”.
Queensland is home to more Papua New Guineans than any other Australian state because of the long history of Papua New Guineans immigrating to Queensland.
The Sugar Slaves
Queensland’s long history of immigration from Papua New Guinea began in the 1870s when Christian Papua New Guinean missionaries and crewmembers first arrived in Australia.
During the early 1880s, labourers from Papua New Guinea came to Queensland to work at, and make, sugarcane plantations. But these labourers did not all come to Queensland by choice. Many came voluntarily, but most were slaves.
Emeritus Professor Clive Moore at the University of Queensland says “5,000” Papua New Guineans were blackbirded, which means they were deceived, tricked, coerced, kidnapped, and bought and sold into indentured servitude.
They were forced to sign contracts which they could not read and sign them with a signature they did not possess. Instead, they used their thumbprint as a signature. They were paid £6 a year and their contracts lasted 3 years.
Before the arrival of the Sugar Slaves, white men were paid £30 a year to do the same work. This rate of £6 a year remained fixed throughout 1863–1901, despite rapid inflation occurring.
The Sugar Slaves were transported in inhumane conditions to Queensland’s bush where they deforested the land and planted, grew, farmed and refined sugarcane. The 5,000 Sugar Slaves from Papua New Guinea were the minority of the Sugar Slaves.
A total 62,500 slaves were blackbirded between 1863–1901. The majority came from Vanuatu and Solomon Islands; the rest came from Milne Bay Provinces in Papua New Guinea, Tuvalu, Kiribati, Fiji, New Ireland, Gilbert Islands, and New Caledonia.
In the 1880s, the Sugar Slaves were finally allowed access to hospital services but in a segregated ward. They were often sick: a third died from exposure to European diseases, malnutrition and mistreatment.
It all ended in 1901 when the new Federal Government of Australia passed the Pacific Island Labourers Act 1901 which was part of the White Australia policy.
The remainder 10,000 Sugar Slaves were deported back to their homes but many Sugar Slaves ended up on the wrong island and a few remained in Queensland and their descendants eventually became a big part of Queensland’s Pacific Islander community.
After the deportations and during the early 1900s, exemptions from the White Australia policies were made for Papua New Guineans who worked in Queensland’s pearl fisheries. This way, the Government controlled which Papua New Guineans worked and lived in Australia.
Malaria internationally
Even though Australia is malaria-free, the rise since 2015 is indicative of the international resurgence of malaria.
Professor Ric Price from the Menzies School of Health Research is a professor of global health, and a senior principal research fellow. He is also a staff specialist in infectious diseases and general medicine at the Royal Darwin Hospital Division of Medicine. His expertise is malaria.
Professor Price says that, “A worrying finding is that for the last three years the global burden of malaria has not fallen and in fact risen as bit. Most of this reversal is in Africa, although a big resurgence is in Papua New Guinea—which is likely due to major issues in supply chain for drugs. In rural areas some clinics have no drugs”
Professor Price confirmed Dr Cameron’s suggestion that most cases of malaria in Australia come from travellers: “Most [cases of malaria] in Australia derive from migrants from Africa screened on arrival and also travellers from Papua New Guinea”.
In World Malaria Report 2018, Director-General of World Health Organization Dr Tedros Adhanom Ghebreyesus corroborated what Professor Price says “the global response to malaria had stalled and we risked losing some of the precious gains we have made over the past 20 years”.
Dr Ghebreyesus also expanded on what Professor Price says about major issues in supply chain for drugs in rural areas: “the level of investment in malaria control remains inadequate”. Dr Ghebreyesus says that the recent lack of investment in malaria control causes “insufficient levels of access to and uptake of lifesaving malaria tools and interventions”.
“Many people who could have benefited from malaria interventions missed out because of health system inefficiencies”.
“Clearly, we need to change course and improve how we combat malaria” Dr Ghebreyesus says. One year after World Malaria Report 2018 was published, how we combat malaria has changed permanently with the first malaria vaccine.
The Malaria vaccine
Malaria kills 435,000 people every year; most of its victims are children.
In Malawi in Africa, the first vaccine—RTS,S—is being given to children under the age of 2.
RTS,S or Mosquirix was developed by
- PATH: Seattle-based international non-profit global health organisation
- GlaxoSmithKline: London-based multinational pharmaceutical company
- The Bill & Melinda Gates Foundation
After Malawi’s children are vaccinated, Mosquirix will be made available to Ghana and Kenya later this year. 360,000 children will be vaccinated every year.
Even though Mosquirix only has a 30%–40% success rate, it is the only malaria vaccine available. To work, the vaccine must be injected four times.
“We need to build on this success. We must double down on malaria and make good on the promise to significantly reduce the global burden of the disease in the next decade. Critically, we must invest in robust health systems that deliver quality services for combating malaria and all diseases” Director-General of World Health Organization Dr Ghebreyesus says.
“I know we can defeat malaria. With the continued commitment of all countries, and the support of development partners, I am confident we will win this fight with this centuries-old disease and get back on track toward our common vision: a malaria-free world”.
Will Atkins
I am a student at UQ studying a bachelor of journalism and a bachelor of arts, majoring in history and English. Check out my instagram for weird/ bad photography. https://www.instagram.com/willatkins1001/